Hep C Discussion Forum
| Chatbox | |
|---|---|
|
Please log in to join the chat!
|
|
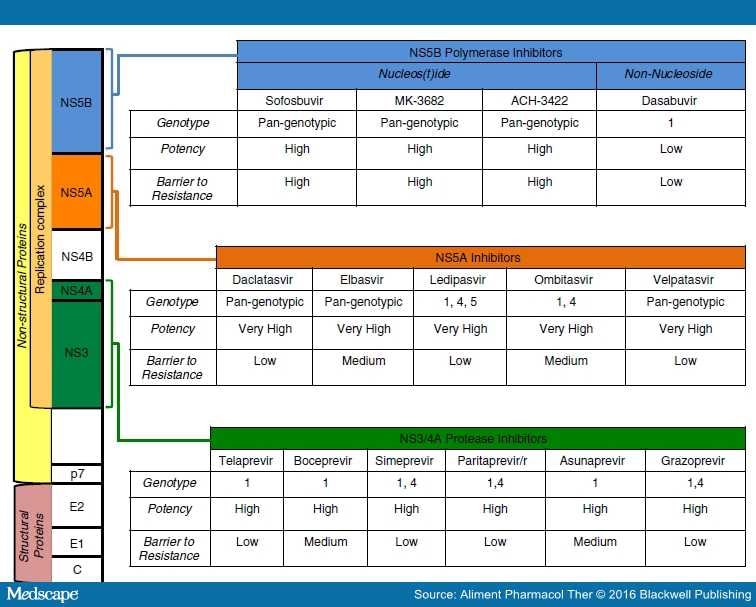
| Post Info | TOPIC: A fairly complete review/synopsis/list - most of the available current HCV drugs | ||||||||
|---|---|---|---|---|---|---|---|---|---|
|
Guru

|
|
||||||||
|
Senior Member

|
|
||||||||
|
Guru
|
|
||||||||
|
Guru
|
|
||||||||
|
Guru
|
|
||||||||
|
Senior Member
|
|
||||||||
|
Guru
|
|
||||||||
|
Guru
|
|
||||||||
|
Senior Member
|
|
||||||||
|
Guru
|
|
||||||||
|
Guru
|
|
||||||||
|
Guru
|
|
||||||||
|
|||||||||






|
|
||
Legal Disclaimer:
THIS FORUM, IT'S OWNERS, ADMINISTRATORS, MODERATORS AND MEMBERS DO NOT AT ANY TIME GIVE MEDICAL ADVICE AND IN ALL CASES REFER ANYONE HERE TO SEEK APPROPRIATE MEDICAL ADVICE FROM THEIR DOCTOR.